




Over the next three months this space will explore concepts of informed self assessment, peer feedback and a continuing competence program that uses these concepts to improve the quality of physiotherapist practice.
This month, a model expressing the dimensions of informed self-assessment is explored. While the model discussed is over decade old, it continues to provide food for thought for health professionals, employers, and regulators on how they might approach using self-assessment and provision of feedback for improving professional practice.
Self-Assessment
One of the defining characteristics of a self-regulating health professional is their ability to self-assess for the purposes of performance improvement.1,2 With this in mind, many health professions regulators have integrated elements of self-assessment into their continuing competence programs.
“Self-assessment is a process of interpreting data about our own performance and comparing it to an explicit or implicit standard”. . . “The power of self-assessment lies in two major domains – the integration of high-quality external and internal data to assess current performance and promote future learning and the capacity of ongoing self-monitoring during everyday clinical practice”1
Most regulators have continuing competence programs that require their members to engage in some type of self-assessment. Most often the benchmark for self-assessment is performance indicators from either a competency profile or standards of practice. The self-assessment activity is written up and submitted for review by the regulator who, in turn, renders a judgment on the member’s submission.4,5
Provision of Feedback
The provision of feedback is much more nuanced than the feedback sandwich (negative comments surrounded by positive comments) commonly described in business blogs.3 Over the years, in an attempt to decrease the anxiety related to feedback, health regulators have adopted compensatory strategies to evolve the way feedback is integrated into continuing competence programs. Some of the strategies commonly used include:
- Providing more objective “data” (i.e., scores and score ranges for multi-source feedback/Physician Achievement Review Program6) and other types of “evidence”
- introducing facilitated feedback
- introducing facilitated feedback from a peer rather than strictly providing results by written communication via letter or email5
The reality is that regardless of the strategy used, the feedback loop never is straightforward and linear. Data to inform self-assessment is never 100% interpreted the way that it is intended. It is not the giving of feedback that is important, it is the receiving and perceiving of feedback that is “more” important and whether what is provided helps nudge members forward to act on the information and use it to work towards better levels of quality practice.
Research and Models
Joan Sargeant5 and her research team were so intrigued by how health professionals reacted to continuing competence results and feedback, they set out to explore how health professionals interpreted and responded to data intended to inform self-assessment. Sargeant interviewed various health-care providers practicing in a number of countries on self-assessment. Their efforts produced a model to explain the variations regulators/educators/employers commonly see in health professionals’ reactions to continuing competence information.
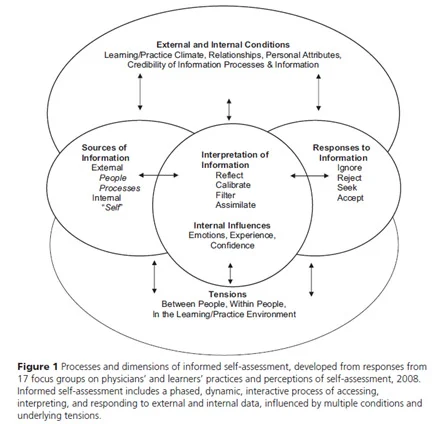
The model was constructed to increase understanding and spearheaded other research into the following five areas:
- Sources of information
- External sources of information (processes [direct and indirect] and people [peers, consultants, other health professionals, supervisors, learners and patients])
- Internal sources of information (the self, emotions, internal state – positive or negative)
- Interpretation of information (how health professionals interpret and critically reflect on external and internal data)
- Responses to information (ignore, reject, seek, accept)
- External and internal conditions (learning/practice climate, relationships to others, credibility of information processes and information, personal attributes)
- Tensions (between individuals, within individuals, in the learning/practice environment)
The research reinforced that:
- Critical and deliberate reflection on assessment and external and internal data is a key activity of the interpretation phase.
- There exist tensions within and between individuals and the environment and these tensions are an integral and inevitable part of self-assessment. For example, within a professional there is fear of learning one is not doing as well as they would like, which is balanced against wanting to know how one is doing.
- If information/data provided is discordant with a professional’s self-identity, it is more likely to be ignored or rejected.
- “The requirement for clear, timely, specific, constructive feedback, preferably offered by trusted, credible supervisors in a safe environment, to inform learners’ self-assessment”5 is essential. As formal feedback from a supervisor is often lacking in the systems health professionals work in, they often turned to their peer networks for feedback.
How does this relate to physiotherapist practice in Alberta?
- Think back to the last time you conducted a self-assessment or received feedback on your performance, is information helpful in explaining how you reacted?
- Self-Assessment against defined benchmarks as a continuing competence strategy was made optional in the College of Physiotherapists of Alberta’s DO.LEARN.GROW. continuing competence program. It wasn’t because self-assessment was not valuable, it was because a one size fits all Self-Assessment Tool in the old program wasn’t working for everyone. In the DO.LEARN.GROW program self-assessment of practice counts as Self-Selected Activity and physiotherapists have the flexibility to develop and use their own assessment tools to benchmark their practice or use the ones the College of Physiotherapists of Alberta has developed.
- Physiotherapists looking for criteria to benchmark their practice should consider using the descriptors found in Competency Profile for Physiotherapists in Canada and the College of Physiotherapists of Alberta’s Standards of Practice. Several tools to support self-assessment of practice have been included on the Self-Selected Activity List (i.e., Essential Competency Self-Assessment, Patient Care Reflection Tool).
- Peers and colleagues can help you assess your performance. Using defined parameters, you can benchmark your performance and peers can provide important source of feedback for ensuring quality practice. Consider innovative and non-threatening ways to involve them to assess your practice.
- Continuing Competence Program requirements in the Health Professions Act are structured such that a summative decision is required regarding whether a member has met or not met the requirements. Consequently, the results letters for the 2020 Self-Selected Activity and College-Selected activity document review provide summative results only. If you would like individualized feedback on the results of your submission contact the competence program staff.
Comments? Contact Continuing Competence Program competence@cpta.ab.ca 780.438.0338, 1.800.291.2782
- Epstein, Ronald M., Daniel J. Siegel, and Jordan Silberman. "Self‐monitoring in clinical practice: a challenge for medical educators." Journal of Continuing Education in the Health Professions 28.1 (2008): 5-13. Accessed 2019 12 04 http://projectes.camfic.cat/CAMFiC/Projectes/Salut_Mental_2010/Docs/_Epstein2008%20Self_MonitoringinClinicalPractice.pdf
- Eva, Kevin W., and Glenn Regehr. "“I'll never play professional football” and other fallacies of self‐assessment." Journal of Continuing Education in the Health Professions 28.1 (2008): 14-19. Accessed 2019 12 04 https://sacme.org/Resources/Documents/Virtual%20Journal%20Club/KWEvaSelfAssessmentJCEHP.pdf
- Hassel, D, 9 ways to give effective employee feedback https://www.15five.com/blog/9-ways-to-give-effective-employee-feedback/
- Paterson, Colin, and Judith Chapman. "Enhancing skills of critical reflection to evidence learning in professional practice." Physical Therapy in Sport 14.3 (2013): 133-138. Accessed 2019 12 04 http://eprints.bournemouth.ac.uk/21394/3/Enhancing%2520skills%2520of%2520critical%2520reflection%2520for%2520BURO.docx.pdf
- Sargeant, Joan, et al. "The processes and dimensions of informed self-assessment: a conceptual model." Academic Medicine 85.7 (2010): 1212-1220. Accessed 2019, 12 04 https://journals.lww.com/academicmedicine/fulltext/2010/07000/The_Processes_and_Dimensions_of_Informed.28.aspx#pdf-link
- Violato C, Lockyer JM, Fidler H. Changes in performance: a 5-year longitudinal study of participants in a multi-source feedback programme. Medical Education. 2008 Oct;42(10):1007–13.


